“We no longer get verbal reports; now everything is documented by the CHPs at the household level. It is encouraging us without a push to do our household visitations.” This sentiment from a Nurse and Community Health Promoter (CHP) captures the transformative impact of the Community Health Promoter Case Report Form (CHP-CRF) which can be found as additional pages in the mother and Child Health (MCH) Book which every mother carries.
For years, County Health Management Teams have grappled with what one Deputy Nursing Officer aptly called “the elephant in the house“—the persistent challenge of documentation at the community level. Services were being delivered, lives were being touched, but without proper documentation, these critical interventions remained invisible in our health systems. This created a blind spot in our health information systems and made it nearly impossible to track the complete journey of mothers through the continuum of care.
The question that kept many of us awake was simple yet profound: How do we bridge this gap between community service delivery and facility-based care?
Bridging the Documentation Divide
The solution – and indeed – innovation lies not just in creating another form, but in its thoughtful integration into existing systems. This form was developed and revised jointly with County and subcounty reproductive health coordinators from six sub counties, as well as County and subcounty community health focal persons from the study areas. Three rounds of piloting were conducted with these stakeholders’ involvement.
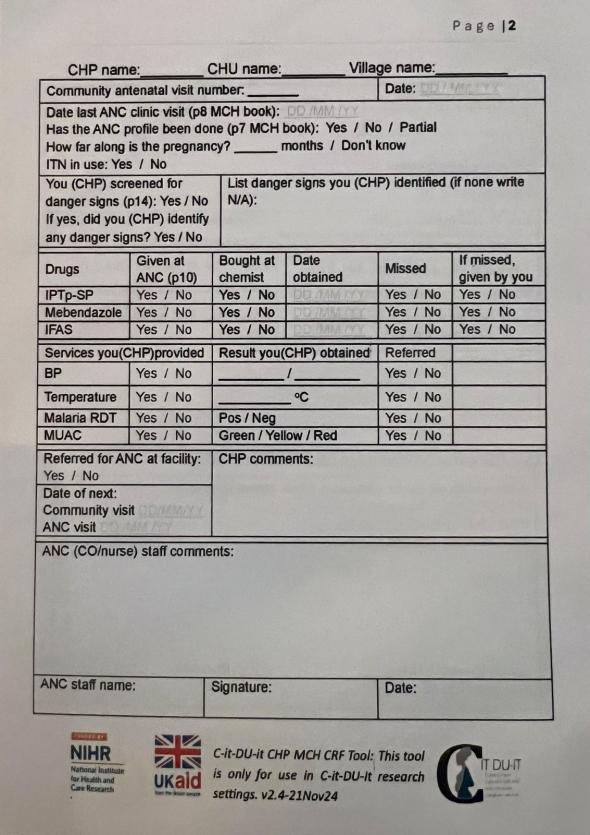
Additionally, consultative meetings were held with County and Ministry of Health stakeholders, where issues such as duplication were addressed before deployment. The form’s design fits neatly into the handheld mother-child booklet and contains a section for Community Health Promoters (CHPs) to complete during home visits, as well as a section for healthcare workers to provide comments after reviewing the CHPs’ entries.
The CHP-CRF has become a seamless part of the documentation tools mothers already carry. It is issued either at the ANC clinic or during home visits, ensuring that every mother’s journey is captured from the very beginning.
Co-Creation: The Foundation of Success
What sets this initiative apart is the deliberate, inclusive approach to its development. Rather than imposing a top-down solution, stakeholders at county, sub-county, and facility levels were brought together to co-create this tool. This wasn’t merely about orientation sessions; it was about genuine engagement—listening to frontline workers, incorporating their insights, and building on their experiences.
This collaborative approach has yielded remarkable results. When you listen to CHPs speak about the form, their passion is palpable. They don’t view it as additional bureaucratic burden but as a tool that validates their work and enhances their professional identity. As one CHP shared in a recent video, the form has fundamentally changed how they approach their work. https://photos.app.goo.gl/zTofjVxjWVELhoCH9
The Evidence Speaks: Multiple Perspectives
The impact of the CHP-CRF resonates across all levels of the health system. For CHPs themselves, the form provides structure and recognition for their work. They report feeling empowered and more professional in their interactions with families. The documentation transforms their role from informal advisors to recognized healthcare providers with accountability and standards.
Healthcare workers at facilities have found the form invaluable for two critical functions: monitoring clients’ journeys through the health system and supervising CHPs. The shift from verbal to written reports has enhanced accountability and made supervision more objective and evidence-based. Supervisors can now track patterns, identify gaps in service delivery, and provide targeted support to CHPs based on documented evidence rather than anecdotal reports.
Perhaps most significantly, mothers themselves are aware of and value the booklet. They understand what is documented within its pages. One mother shared a particularly poignant insight: “It even allows the doctor to see the things I am afraid of telling them.” This reveals how the form serves as a communication bridge, enabling more comprehensive care by capturing information through trusted community health promoters, that might otherwise remain hidden due to fear, stigma, or forgetfulness.
Addressing Concerns and Moving Forward
While the enthusiasm is encouraging, County Health Management Teams have rightly raised concerns about sustainability. Will this initiative face the same documentation challenges that have plagued other programs? The key to avoiding this pitfall lies in recognizing that the CHP-CRF is not just another form—it’s a cultural shift in how we value and capture community-level health work.
Some have noted that similar documentation exists in the MCH booklet[FO5] . However, the CHP-CRF fills a specific gap: it documents the CHP’s activities, observations, and interventions at the household level before and between facility visits. It captures the invisible work happening in homes across our counties, work that is critical to maternal and child health outcomes but has historically remained undocumented.
The Path Forward
For County Health Management Teams, the CHP Case Report Form represents an opportunity to finally solve the documentation challenge that has frustrated us for years. It provides accountability without creating unmanageable burden. It motivates CHPs by recognizing their work. It improves continuity of care by ensuring information flows seamlessly from community to facility and back.
The “silent supervisor” is working—not through enforcement or punishment, but through empowerment and recognition. When CHPs say the form encourages them “without a push” to complete household visitations, we know we have found something that aligns professional standards with intrinsic motivation.
As we scale this innovation across counties, let us remember that its success lies not in the form itself, but in the collaborative spirit that created it and the genuine value it provides to all stakeholders—from CHPs to healthcare workers to the mothers and children we serve.
We are slowly bridging the gap and documentation at the community level is becoming a reality, one household visit at a time.


